Retinopathy of Prematurity and Its Association with Oxygen Therapy in Preterm Low Birth Weight Babies
Mandal AA1*, Nahar K2, Hosneara3, Mazid AHMR4, Yesmin N5
DOI:https://doi.org/10.17511/ijpr .2025.i03.02
1* Abul Azad Mandal, Senior Consultant (Pediatrics), General Hospital, Gaibandha, Bangladesh.
2 Khairun Nahar, Junior Consultant (Pediatrics), General Hospital, Gaibandha, Bangladesh.
3 Hosneara, Junior Consultant (Pediatrics), Aminbazar 20 Bed Hospital, Savar, Dhaka, Bangladesh.
4 Abu Haider Md Raziul Mazid, Medical Officer (Pediatrics Haemato-Oncology), General Hospital, Gaibandha, Bangladesh.
5 Nafisa Yesmin, Assistant Professor (Pediatrics Haemato-Oncology), Rangpur Medical College, Rangpur, Bangladesh.
Background: Retinopathy of prematurity (ROP) is a preventable cause of blindness in premature, low birth weight (LBW) infants, driven by abnormal retinal vascular development. Oxygen therapy, though life-saving, is a key modifiable risk factor when unmonitored, leading to retinal damage through disrupted angiogenesis. ROP follows a two-phase pathogenesis involving initial vessel growth suppression due to hyperoxia, followed by hypoxia-induced neovascularization. In countries like Bangladesh, rising preterm survival without adequate neonatal care infrastructure has increased ROP incidence.
Methods: This cross-sectional observational study was conducted in the NICU of Pediatrics Dept., General Hospital, Gaibandha in Bangladesh to assess the prevalence of ROP and its association with oxygen therapy among 50 preterm, low-birth-weight infants. Eligible neonates (<37 weeks, <2500g, oxygen-exposed, and screened for ROP) were enrolled over a defined study period of January to June 2023. Data were collected using structured forms covering clinical, demographic, and treatment details. ROP screening followed standard protocols using indirect ophthalmoscopy. Oxygen therapy mode and duration were recorded. Statistical analysis was performed using SPSS v26.0, applying descriptive statistics and chi-square/Fisher’s exact tests, with significance set at p < 0.05.
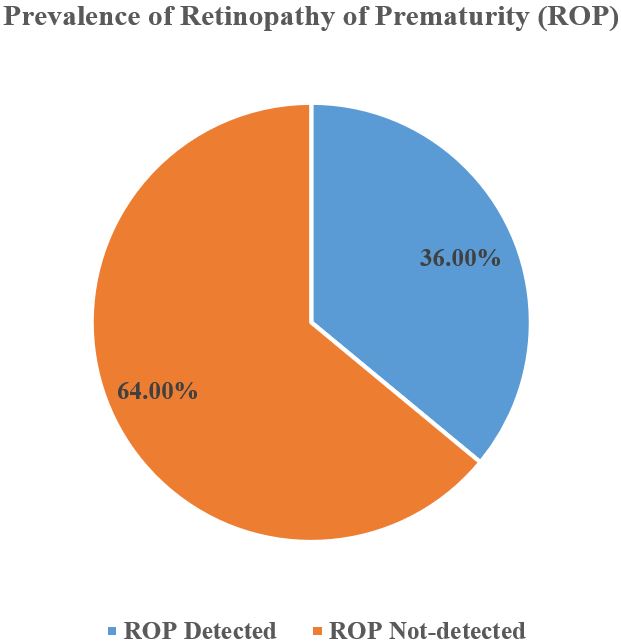
Results: Among 50 preterm low birth weight infants, 36% developed retinopathy of prematurity (ROP). Most were male (56%), born at 28–31 weeks (48%), and weighed 1000–1499 g (64%). CPAP was the most common oxygen modality (48%), with a mean oxygen duration of 5.8±2.3 days. ROP primarily involved Zone II (61.1%) and Stages 1–2. Bilateral ROP occurred in 61.1%, and 50% of cases required treatment. A significant association was found between oxygen therapy and ROP (p=0.04), especially with prolonged exposure (≥5 days; p=0.02) and mechanical ventilation (p=0.03), highlighting oxygen therapy as a key risk factor for ROP development.
Conclusion: This study highlights a significant association between unregulated oxygen therapy and ROP in preterm, low-birth-weight infants. Improved oxygen monitoring, adherence to saturation targets, and early ROP screening are essential to prevent vision loss. Strengthening neonatal care protocols can reduce the burden of this preventable cause of childhood blindness.
Keywords: Retinopathy of Prematurity, Oxygen Therapy, Preterm Infants, ROP Screening and Premature Birth
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Consultant (Pediatrics), , General Hospital, Gaibandha, , Bangladesh. Email:  |
Mandal AA, Nahar K, Hosneara, Mazid AHMR, Yesmin N, Retinopathy of Prematurity and Its Association with Oxygen Therapy in Preterm Low Birth Weight Babies. Pediatric Rev Int J Pediatr Res. 2025;12(3):63-69. Available From https://pediatrics.medresearch.in/index.php/ijpr/article/view/805 |
 |
 ©
©